The answer is “nothing.” You are required to do PQRS measures on over 50% of your traditional Medicare covered patients to assess for all manner of problems in addition to your typical clinical focus in the appointment. You must document in the chart what was done and any follow-up (referrals, treatment, etc.) results and then you must bill those procedures on your HCFA 1500 at $0.01 each because some billing programs won’t accept $0.00.
Recognize that each measure can have many CPT procedure codes attached to it. For example if you give Measure #131 Pain Assessment and Follow-Up by administering a standardized pain assessment tool there are six possible outcomes for which you could bill six different CPT codes, depending on what you document in the medical record; these options include findings that were:
• Negative-no follow-up plan required then you bill CPT code: G8731 for $0.01 on your HCFA 1500 or electronically.
• Positive–follow-up plan included referral to a specialist and short-term medication… you bill code G8730.
–or–
• Positive–but a follow-up plan is not documented as the patient was not eligible (e.g., in hospice care) for follow-up care which you must document. You bill G8939.
• Unknown–no documentation for a pain measure is needed as the patient is not eligible (e.g., s/he in a coma) which must be documented. You bill G8442.
–or–
• Unknown–no documentation of any pain measure given, no reason offered/documented. You bill G8732.
• Positive–but a follow-up plan is not documented and no reason for this offered/documented. You bill G8509.
It is unlikely that you would every bother to bill the last two codes, G8732 or G8509 since these do not count as valid PQRS measure administrations. CMS says the PQRS measure #131 performance was not met adequately to count, basically due to absent or poor documentation. But, if you do the measure and don’t document a follow-up plan because the patient was ineligible to benefit from follow-up (e.g., they are in hospice on end of life drug therapy) you can still bill G8939 and get credit. –or– You tried but couldn’t do the measure because the patient was in a coma which you document, then you can bill G8442, and get credit for doing PQRS measure #131.
So there are hundreds of measures you can choose from and many options to bill for each measure, which astronomically increases the complexity of your Super Bill, as for each measure there can be several (like the six billing options above) CPT codes of which some count and some don’t towards your PQRS count, and none of which will pay anything. My HCFA 1500’s may have a single diagnostic or treatment procedure on them followed by 7 to 9 additional CPT codes for various PQRS measures billed at $0.01. But wait it gets far more complex, time consuming and even more costly in lost income for time spent! CMS prefers certain clusters or groups of measures in some clinical specialities. For example, the Neuropsychology group includes 9 different measures–the good news is if you do them all they and they are all negative, then they can be billed as a single cluster CPT code! The bad news is you still have to do 9 separate measures. More bad news: if any of them are positive and need a treatment plan, then you have to bill them all separately. I may have to study several dozen CPT code options to bill all 9 measures and It can take two HCFA 1500 forms to bill for a single procedure.
All of this just to prove to CMS that various areas are being screened beyond your practice area of specialty. The penalties add up to about 5% deduction in your allowed rate. Add that to the 2% already deducted by the sequester process when the Congress failed to consummate a grand budget, and you can face a not insignificant 7% reduction in gross Medicare income in 2017.
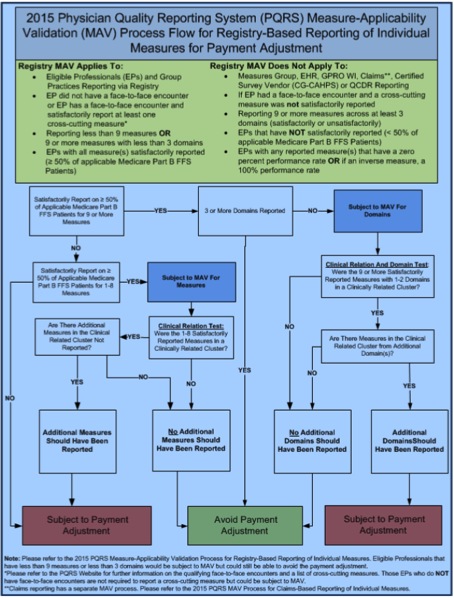
Yet, there is still more–this is special. For some PQRS measures, CMS can only be notified that you did them through an on-line registry which you have to pay and then add steps for your billing staff to communicate the measures you give. I could go on and on, but I think the description of just one component of this CMS-induced nightmare serves to show you the complexity of just the MAV procedure to determine if you did 9 measures across 3 domains, check it out and see if the following flow-chart makes sense to you:
Fortunately, there are methods to help which actually allow a provider such as a physician, NP or PA to get paid to do screenings and assessments in areas supplemental to their typical clinical focus. This is where TestSTAT comes into the picture.